
Research Article
Knowledge and Perception of Preventable Medical errors in Sultanate of Oman
School of Pharmacy, College of Pharmacy and Nursing, University of Nizwa, Oman
*Corresponding author: Jamaluddin Shaikh, Associate Professor, School of Pharmacy, College of Pharmacy and Nursing, University of Nizwa, Oman, E-mail: jamaluddin@unizwa.edu.om
Received: December 27, 2018 Accepted: January 21, 2019 Published: January 28, 2019
Citation: Shaikh J, Al-Ruzaiqi HS. Knowledge and Perception of Preventable Medical errors in Sultanate of Oman. Madridge J Nurs. 2019; 4(1): 134-138. doi: 10.18689/mjn-1000124
Copyright: © 2019 The Author(s). This work is licensed under a Creative Commons Attribution 4.0 International License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Background: Medical errors are responsible for numerous issues which include decreased effectiveness of medical services, added responsibility and financial overload, legal dispute and harmful effects of the medical services to the patients. Available reports indicated that people have negative impacts when medical errors lead to serious health problems. The aim of this study is to assess the public knowledge and perceptions about the medical errors and to identify the reasons behind these problems in different Governorates in Sultanate of Oman.
Methodology: This study was carried out in different Governorates in Sultanate of Oman during 2015-2016 among general public. A self-administered questionnaire was developed that had questions to obtain information based on the objectives of the study. It had a component to obtain information on demographics of the participants as well. Both Omani and non-Omani public (males and females) were participated. Data were collected to evaluate the reasons for medical errors, and to explore general peopleʼs perceptions about it. The obtained responses were correlated with the demographics of the participants.
Results: Among the three hundred fifty participants, majority were males (69%) and in the age group of 21-30 years. Most of the respondents were bachelor graduates (60%), and were employed in the government sectors (75.8%). When asked about the knowledge of medical errors, about half of the respondents agreed that medical errors were very common in Oman. When enquired about the reasons for medical errors, majority of the participants strongly agreed that it is usual for patients to be given the wrong medicines and there is lack of transparency to fix the problems. When asked if they have been gone through medical errors, half of the participantʼs responded affirmative (49.6%). When enquired about the reasons, majority of the participants responded that prescribing, dispensing and administering wrong medicines (31.4%) and poor performance of medical staff and health care workers (36.3%) were the major contributing factors for medical errors.
Conclusion: It was observed that a large percentage of participants have been passed through medical errors. Due to the appropriate education and recent health awareness, majority of participants had knowledge on what is a medical error, type of medical error and reasons for medical error. The implementation of information technology in prescribing, labeling and dispensing of medicines is essential. It is the duty of healthcare professionals to adopt constructive strategies to avoid medical errors.
Keywords: Medical errors; Knowledge; Perception; General public; Causes of medical errors.
Introduction
The stories of medical errors are abundant in the society. It is an avoidable untoward effect of service, irrespective of noticeable or dangerous, to the patient. In other words, medical errors occur when a healthcare institution or healthcare provider involves in incorrect or insufficient diagnosis or medical care of a disease, injury, syndrome, contamination, infection, or other illness [1]. Researchers indicated that medical errors around the globe are growing every year. A recent study from US showed that medical errors are one of the major causes of death after cardiovascular disease and cancer [2]. Another study from US estimated that at least 1.5 million patients are suffering from medical errors per year [3].
Medical errors related cost in the United States was estimated $19.5 billion in 2008. Andel et al. evaluated that the financial impact was costly, probably about $1 trillion per year when quality-adjusted life years were connected with those that die [4]. Medical errors reported to include prescribing, dispensing and administering medicines, lack of knowledge about the patient, communication gaps between healthcare provider and the patient, system inaccuracy, inappropriate documentation, inadequate performance of medical staff like doctors, nurses and pharmacists, poor physician-to-patient ratios, insufficient nurse-to-patient ratios, sound-alike drugs, and improper use or acceptance of technology in the health care institutions [5-7].
Available studies stated that irrational and inappropriate prescribing was the main contributing factor among commonly occurring medical errors [8-10]. In numerous occasions, prescribing errors are harmful to patients. They are one of the crucial sources of morbidity and mortality in patients [11,12]. The most common factors that are associated with prescribing errors include added workload, adverse and stressful working environment, communication gaps among healthcare personnel, lack of knowledge and skills in prescribing and less experience [13].
Medical errors, particularly those caused by a communication failure, are a common problem in todayʼs healthcare systems [14-17]. Errors can develop as a result of communication gaps among medical staffs. Medical errors that develop from nurses include dispensing medication far away from permissible instruction, dispensing the wrong medication because of sound-alike name or appearance, paying less attention to the instruction printed on the package, and unnecessary late in drug dispensing [18,19]. Errors that initiate by doctors include scribbled handwriting, inaccurate dose and route of administration of drugs, and not verifying the patient identification or bed number [19].
Patients also contribute to the medical errors when they are not honest with the doctor about their health status, and when they delay or ignore symptoms which could be associated with chronic disease, or when they are not providing all of their information to healthcare providers which is related to the symptoms, currently used drugs, information about allergies and concomitant diseases [6].
Medical errors are also occurred due to inexperienced health care providers due to lack of new techniques, and complex or emergency care [20]. About 80 percent of adverse effects in complex healthcare facilities are due to human errors. Inaccurate systems and unacceptably designed procedures also contribute to vast majority of medical errors [21].
Information technology systems in medication management are very common nowadays. It helps both physicians and patients. Many countries in the world are using medical technology to minimize medical errors. The United States use many technologies like an electronic medical records, Bar code eMAR technology which assure that the accurate drug is dispensed in the exact dose at the appropriate time to the right patients. Application of this system helps patients to communicate with their physicians in organized manner [22]. Technology is playing a big role in the Omani healthcare systems also. Healthcare facilities are using the latest equipment and systems. Hospitals and medical centers in Oman are automated with ALSHIFA system, a comprehensive healthcare service management system adopted by Ministry of Health (MOH) hospitals and health centers [23].
However, a recent review confirmed that discrepancies with health-related IT system can disorganize healthcare facility and injure patients. The outcome from this review was qualitative. In addition to its benefits to patient safety, this review also quantify IT risks [24]. Some of the effects of IT problems on clinical errors may include medication errors in administration and lack of success to follow up diagnostic outcomes. Gaps in healthcare system were associated with facility access [25,26] and issue of software effectiveness. The success of software is compromised with defective user interfaces and fragmented displays [27]. Updates on software, were also outlined to influence healthcare system [28,29].
Hence, to repair the gap in medical practice, this study was carried out with the aim to assess the knowledge and perception of the general public on medical errors. Moreover, there are not many studies conducted in Sultanate of Oman regarding this issue. Therefore, the need of the present study is to generate better knowledge and perception towards preventable medical errors. This study may help the existing organizations, government and MOH to take advantages of these observations to minimize medical errors to establish a healthy society.
Materials and Methods
This is a prospective study with the use of questionnaires to collect data from different Governorates of Sultanate of Oman. The consent was obtained verbally from all the subjects before registering their response. The survey questionnaire was given to both Omani and non-Omani general public, both males and females. Age between 21 to 70 years was the inclusion criteria. The questionnaire was written in both English and Arabic languages, the English was for non-Omani public and Arabic (the local language) was for Omani public. Participants who were unwilling to participate in the study and mentally disabled persons were excluded in the present study. This study was adapted pretested structured questionnaire to assess the publicʼs knowledge, and perception about medical errors. The study was conducted during 2015-2016 by using self-administered questionnaires that included demographic parameters and questions about the knowledge and perception of medical errors. Participantʼs demographic parameters were also used in this study. The participantʼs cultural parameters include employment and education. Directly related questions associated to the knowledge of medical errors were included. The questionnaires related to perception include abundances, impacts and reasons behind medical errors.
350 general public were participated in the survey. The questionnaire was reviewed by the authors and relevant colleagues from the College of Pharmacy and Nursing Research Committee, University of Nizwa. Also a pilot-study was carried out to test the clarity, simplicity, and reasonability of questionnaire on a sample of general public and revised accordingly. All the obtained data were analyzed and illustrated in histograms using Microsoft Excel programs.
Results
The present study was carried out in different Governorates in Sultanate of Oman for both sexes. 28.6% of the study population were from Muscat (the capital), followed by 21.7% from Al-Sharqiya, 21.1% from Al-Dakhiliah, 13.2% from Al-Batinah, 4.6% from Dhofar, 4% from Al-Dhahirah, and 3.4% each from Al-Wusta and Al-Burayimi Governorates. Among the participated general public, the percentage of males (69%) were more than females (31%). The level of education of respondents ranged from no education to higher degree holders. Sixty percent (60%) of them had obtained university graduation, followed by those with diploma degree holders (21.4%), secondary education (8.3%) and primary education (7.2%), while 3.1% had received no formal education. Most of the participantʼs age in the present study was between 21 to 50 years (age groups 21-30, 31-40 and 41-50 were 31%, 30% and 21% respectively). Regarding employment status, majority of the participants were government employee (75.8%) followed by university students (16.5%).
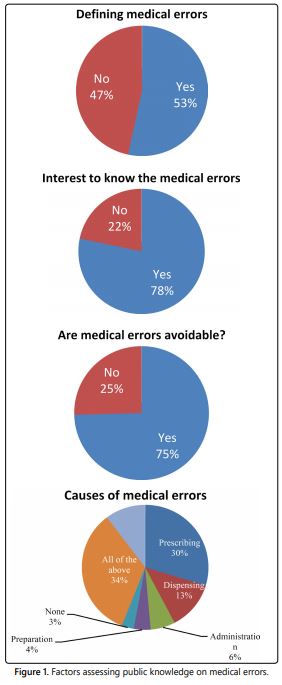
In the present study, survey respondents were asked if they had knowledge about medical errors. The results indicated that majority (53.4%) of respondents had heard about the medical errors. Most (78.3%) of the respondents were eager to know the medical errors (Figure 1). This figure also showed that about three-fourth (74.6%) of the respondent evaluated medical errors to be a preventable event.
The factors that contribute to evaluating the general public knowledge about causes of the medical errors are also shown in figure 1. It showed that prescribing errors (29.7%) were thought to be the major causes of medical errors followed by dispensing (12.6%), administration (6.3%) and preparation (4.3%). About one-third of the respondents (33.7%) had a belief that all of the above-mentioned types of errors can lead or considered as medical errors.
The majority of survey respondents (49.6%) pointed out that medical errors create serious threats to individuals, whereas a small portion (17.4%) consider error was not a threat. Three-fourth (73.4%) of the respondents disclosed that medical errors would surge their healthcare burden. Majority (81.7%) of the respondents indicated that medical errors reporting system should be established to overcome the issue (Figure 2).
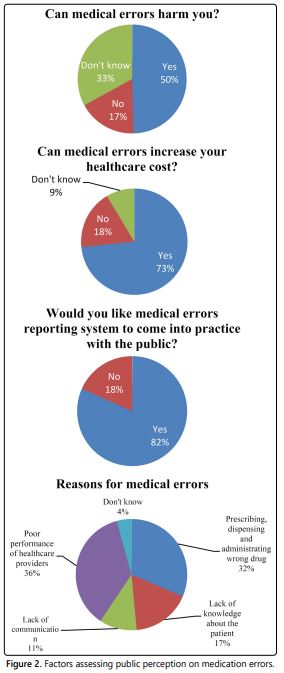
The perception of respondents about the reasons for medical errors indicated that poor performance of medical staff or healthcare providers (36.3%) were perceived to be contributing the maximum towards the incidence of medical errors, followed by prescribing, dispensing and administrating wrong medicines (31.4%). Lack of knowledge about the patients (17.1%), and lack of communication between medical staffs and the patients (10.9%) also contribute to the medical errors (Figure 2).
Discussion
This study was designed to identify the medical errors in Oman together with the investigation of reasons of medical errors and how these errors affecting Oman. Upon evaluation of the demographic details of the participants who were enrolled in this study, it was observed that the majority of them were males (69%) and in the age group of 21-30 years. Most of the participants were bachelor degree holders (42.3%). Also considering the evaluation of employment status of the respondents, the majority of the participants were employed in the government sectors (42.3%).
It was observed that when asked about their level of knowledge on defining medical errors, majority of the respondents acknowledged their understanding (53.6%) about the issue. Also it was observed that when asked about their knowledge on causes respondents were able to identify the factors responsible for medical errors. The reflection of response could be due to the appropriate education and health awareness of the respondents.
The present study indicated that prescribing errors (29.7%), as per the knowledge of the respondents, were the major causes of medical errors followed by dispensing (12.6%), administration (6.3%) and preparation (4.3%). Moreover, about one-third of the respondents (33.7%) had an understanding that combinations of above-mentioned types of errors could lead to medical errors. Overall, the findings concluded that general public had a good knowledge about the causes of medical errors. Our observations are in line with a recent observation by Ponnusankar et al. [30].
When asked if they have been through a medical error, the majority of respondents answered affirmative (49.6%); when enquired about the reasons, majority of the respondents acknowledged that prescribing, dispensing and administrating wrong medicines (31.4%) and poor performance of medical staff and health care providers (36.3%) are the main reasons for medical errors. This may be due to stress, and busy schedule of healthcare provider, which force them to prescribe wrong medications [20]. Patients are also contributing to the errors when they are not being honest with the doctor about their health status, delaying or ignoring symptoms which may be related to a chronic disease, and not giving all the information which is related to the symptoms, the medicine use, allergies and any comorbidity [6]. Lack of communication between healthcare provider and patient is also important contributing factor. The healthcare professionals can improve public impression and trust by admitting errors to patients, devoting more time to patients, and communicating carefully [31].
It was found that young adults aged between 21-30 years, female and graduates had a better level of knowledge, and perception of medical errors. The important finding in the present study was to observe that medical error is very common in Oman. As per the obtained data is concerned, it is usual for patients to be given the wrong medicine, and lack of transparency to fix the issues is one of the challenges to rectify the medical errors.
Conclusions
This study was carried out among the general public in different Governorates in Sultanate of Oman. The questionnaire distributed to both Omani and non-Omani individuals. As like global trend, medical errors still remain threat to the healthcare system in Oman also. Hence, it is important to strengthen the understanding of general public about the reasons, and complications toward medical errors. Due to appropriate education and recent health awareness majority of the respondents had knowledge on medical errors. The collected information may help in describing and translating an idea about the knowledge and perception of general public towards the preventable medical errors. To minimize these events, establishing an effective and a reliable reporting system is necessary. Therefore, the transformation of information technology in prescribing, labeling and dispensing of medicines is essential to know and prevent co-occurrence of medical errors. Also, the healthcare professionals should adhere to their duties in effective and careful manner to avoid errors.
Acknowledgments
We would like to express our thanks and gratitude to the University of Nizwa and the College of Pharmacy and Nursing for giving this opportunity to conduct this research via the provision of the academic programs. Our thanks are also extended to the respected respondents without their kind response this study cannot be conducted.
Declaration of Conflicts of Interest
The authors declared no conflicts of interest with respect to the authorship and/or publication of this.
References
- Institute of Medicine (US) Committee on Quality of Health Care in America. To err is human: building a safer health system. National Academies Press (US); 2000.
- Makary MA, Daniel M. Medical error-the third leading cause of death in the US. BMJ. 2016; 353: i2139. doi: 10.1136/bmj.i2139
- Aspden P, Wolcott JA, Bootman JL, Cronenwett LR. Preventing medication errors. Washington, DC: National Academies Press; 2007.
- Andel C, Davidow SL, Hollander M, Moreno DA. The economics of health care quality and medical errors. J Health Care Finance. 2012; 39(1): 39-50.
- Friedman RA. CASES; Do Spelling and Penmanship Count? In Medicine, You Bet. The New York Times. 2003.
- Grober ED, Bohnen JM. Defining medical error. Can J Surg. 2005; 48(1): 39-44.
- Hayward RA, Hofer TP. Estimating hospital deaths due to medical errors: preventability is in the eye of the reviewer. JAMA. 2001; 286(4): 415-420. doi:10.1001/jama.286.4.415
- Kozer E, Scolnik D, Macpherson A. Variables associated with medication errors in pediatric emergency medicine. Pediatrics. 2002; 110(4): 737-742.
- Ghaleb MA, Barber N, Franklin BD, Yeung VW, Khaki ZF, Wong IC. Systematic review of medication errors in pediatric patients. Ann Pharmacother. 2006; 40(10): 1766-1776. doi: 10.1345/aph.1G717
- Lesar TS, Lomaestro BM, Pohl H. Medication-prescribing errors in a teaching hospital: a 9-year experience. Arch Intern Med. 1997; 157(14): 1569-1576.
- Al-Dhawailie AA. Inpatient prescribing errors and pharmacist intervention at a teaching hospital in Saudi Arabia. Saudi Pharm J. 2011; 19(3): 193-196. doi: 10.1016/j.jsps.2011.03.001.
- Tam VC, Knowles SR, Cornish PL, Fine N, Marchesano R, Etchells EE. Frequency, type and clinical importance of medication history errors at admission to hospital: a systematic review. CMAJ. 2005; 173(5): 510-515. doi: 10.1503/cmaj.045311
- Dean B, Schachter M, Vincent C, Barber N. Causes of prescribing errors in hospital inpatients: a prospective study. Lancet. 2002; 359(9315): 1373-1378. doi: 10.1016/S0140-6736(02)08350-2
- Smith IJ. The Joint Commission guide to improving staff communication. Joint Commission Resources. 2005.
- Allard J, Carthey J, Cope J, Pitt M, Woodward S. Medication errors: causes, prevention and reduction. Br J Haematol. 2002; 116(2): 255-265. doi: 10.1046/j.1365-2141.2002.03272.x
- Maxfield D, Grenny J, McMillan R, Patterson K, Switzler A. Silence Kills: The Seven Crucial Conversations for Healthcare. Provo, UT: Vital Smarts LC; 2005.
- McNutt RA, Abrams R, Aron DC. Patient safety efforts should focus on medical errors. JAMA. 2002; 287(15): 1997-2001.
- Weingart SN, Wilson RM, Gibberd RW, Harrison B. Epidemiology of medical error. BMJ. 2000; 320(7237): 774-777.
- Palmieri PA, DeLucia PR, Peterson LT, Ott TE, Green A. The anatomy and physiology of error in adverse health care events. Patient Safety and Health Care Management. 2008; 7: 33-68. doi:10.1016/S1474-8231(08)07003-1
- Poon EG, Keohane CA, Yoon CS, et al. Effect of bar-code technology on the safety of medication administration. N Engl J Med. 2010; 362: 1698-1707. doi: 10.1056/NEJMsa0907115.
- Al-Gharbi K, Gattoufi SM, Al-Badi AH, Al-Hashmi A. A Case Study of AlShifa: A Healthcare Information System in Oman. International Journal of Humanities and Social Sciences. 2014; 8(8): 2451-2456.
- Kim MO, Coiera E, Magrabi F. Problems with health information technology and their effects on care delivery and patient outcomes: a systematic review. J Am Med Inform Assoc. 2017; 24(2): 246-250. doi: 10.1093/jamia/ocw154
- Warm D, Edwards P. Classifying Health Information Technology patient safety related incidents–an approach used in Wales. Appl Clin Inform. 2012; 3(2): 248-257. doi: 10.4338/ACI-2012-03-RA-0010
- Lei J, Guan PC, Gao K, et al. Characteristics of health IT outage and suggested risk management strategies: An analysis of historical incident reports in China. Int J Med Inform. 2014; 83(2): 122-130. doi: 10.1016/j.ijmedinf.2013.10.006
- Koppel R, Metlay JP, Cohen A, et al. Role of computerized physician order entry systems in facilitating medication errors. JAMA. 2005; 293(10): 1197-1203. doi: 10.1001/jama.293.10.1197
- Aarts J, Doorewaard H, Berg M. Understanding implementation: the case of a computerized physician order entry system in a large Dutch university medical center. J Am Med Inform Assoc. 2004; 11(3): 207-216. doi: 10.1197/jamia.M1372
- Landman AB, Takhar SS, Wang SL, et al. The hazard of software updates to clinical workstations: a natural experiment. J Am Med Inform Assoc. 2013; 20(e1): e187-e190. doi: 10.1136/amiajnl-2012-001494
- Ponnusankar S, Roy RR, Babu S, Mohamed EB, Cyril S, Kamal M. A Descriptive Cross-Sectional Study on the Assessment of Public Knowledge, Attitude and Perception on Medication Errors. Indian Journal of Pharmacy Practice. 2017; 10(4): 282-286. doi:10.5530/ijopp.10.4.57
- Northcott H, Vanderheyden L, Northcott J, et al. Perceptions of preventable medical errors in Alberta, Canada. Int J Qual Health Care. 2008; 20(2): 115-122. doi: 10.1093/intqhc/mzm067
