

Research Article
Evaluating Outcomes of Supportive Care on the Quality of Life of Cancer Patients: Study Design and Rationale
1 Department of Radiation Oncology, All India Institute of Medical Sciences, Rajasthan
2 Department of Surgical Oncology, All India Institute of Medical Sciences, Rajasthan, India
3 Department of Medical Oncology, All India Institute of Medical Sciences, Rajasthan, India
4 Department of Psychiatry, All India Institute of Medical Sciences, Rajasthan, India
5 Department of General Medicine, All India Institute of Medical Sciences, Rajasthan, India
6 Senior Dietician, All India Institute of Medical Sciences, Rajasthan, India
7 Department of Physical Medicine and Rehabilitation, All India Institute of Medical Sciences, Rajasthan, India
8 Department of Community Medicine and Family Medicine, All India Institute of Medical Sciences, Rajasthan, India
9 Department of Nursing, All India Institute of Medical Sciences, Rajasthan, India
10Department of Pediatrics, All India Institute of Medical Sciences, Rajasthan, India
*Corresponding author: Puneet Pareek, Department of Radiation Oncology All India Institute of Medical Sciences, Jodhpur, Rajasthan India, E-mail: drpuneetpareek@gmail.com
Received: January 31, 2023 Accepted: March 07, 2023 Published: April 07, 2023
Citation: Pareek P, Vishnoi JR, Vyas RK, Devnani B, Solanki A, Poonia D et al. Evaluating Outcomes of Supportive Care on the Quality of Life of Cancer Patients: Study Design and Rationale. Madridge J Cancer Stud Res. 2023; 5(1): 103-107. doi: 10.18689/mjcsr-1000115
Copyright: © 2023 The Author(s). This work is licensed under a Creative Commons Attribution 4.0 International License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Cancer and its treatment cause a plethora of symptoms and side effects in cancer patients. These factors contribute to a lower quality of life (QoL) and a greater need for supportive care for cancer patients. In India, where the cancer burden is high, the QoL of cancer patients has received insufficient attention. To fill this gap, the Comprehensive Cancer Patient Support Services (CPSS) program was initiated at the Centre of Excellence of AIIMS, Jodhpur, to provide supportive care (psychological counseling, nutrition counseling, physical and rehabilitation services, palliative care, and social welfare services) to adult cancer patients under one roof alongside conventional treatment. A study has been planned to evaluate the outcomes of this holistic care approach. The primary objective of this study will be to analyze the impact of the approach being followed under the CPSS program on patients’ QoL. The findings of this study will provide insights into the potential impact of cancer and its treatment on patients’ functioning and well-being, as well as identify prevalent difficulties that patients confront, and propose relevant interventions to address these problems in Indian settings.
Keywords: Cancer, Supportive Care, Holistic Care, Quality of Life, EORTC QLQ, Palliative Care, Rehabilitation, Psychological Counseling, Nutritional Support
Abbreviations:
CoE: Centre of Excellence
CPSS: Comprehensive Cancer Patient Support Services
QoL: Quality of life
EORTC: European Organization for Research and Treatment of Cancer
QLQ-C30: Quality of Life Questionnaire Core 30 Items.
OPD: Outpatient department
Introduction
Cancer is one of the most common causes of death across the globe [1]. According to the GLOBOCAN cancer statistics, there were about 19.3 million new cases of cancer worldwide in 2020 with over 10.0 million deaths [2]. Similarly in India, cancer is a huge public health concern with about 1.32 million new cases and roughly 0.85 million deaths occurring in 2020 [3]. With the disease burden increasing year after year, the number of cancer cases is expected to rise by 12% by 2025 [4].
Cancer has a profound impact on patients, their families, and survivors [5]. Patients diagnosed with cancer need additional medical information regarding their disease as well as the benefits and drawbacks of the various therapeutic options available to them [6,7]. Cancer patients need total clinical care for their physical conditions as well as the treatment-related side effects [6,8]. Additionally, these patients frequently seek support in coping with emotional and psychological problems [6,7]. Malnutrition is common in cancer patients as cancer treatments have a major impact on patients’ nutritional requirements [9]. Poor adherence to cancer treatment is another common and important issue that affects clinical outcomes [10]. Importantly, these supportive care needs of cancer patients are mostly not identified or met.
It has been reported that cancer can influence all aspects of a patient’s quality of life (QoL) [5]. The decline in QoL begins after the diagnosis of cancer and continues to increase due to the aggressive nature of the treatment [11]. Long-term cancer therapy is associated with numerous undesirable side effects that cause enormous distress in patients and lower their overall QoL [5,11]. Therefore, the assessment of the QoL of cancer patients is crucial for planning efforts to improve patients’ well-being.
Rationale of the Study
In Oncology, the necessity of maintaining or improving patients’ QoL throughout the cancer journey is becoming better recognized [5,12,13]. One strategy to improve patients’ QoL is to provide supportive care [13,14]. According to reports, cancer patients’ unmet supportive care needs are linked to low QoL, and meeting these needs improves their QoL [9,14]. A prospective cohort study conducted in Germany found that adult patients with breast or gynecological cancer, at the start of a hospital-bound rehabilitation program that included medical therapy, physiotherapy, psychological counseling, and diet counseling, among other therapies, had significant supportive care needs. However, all unmet needs were significantly reduced at the end of the rehabilitation program. Furthermore, meeting the supportive care needs of patients was linked to improved QoL in all the functional domains studied [14]. In addition to enhancing QoL, supportive care has been demonstrated to promote the continuation of therapy and optimize therapy outcomes in cancer patients [15]. According to a study conducted in a hospital in Paris, supportive care measures improved outpatient follow-up, in turn, reduced the occurrence of chemotherapy-related side effects, treatment cancelations and modifications, chemotherapy wastage, and length of stay in the outpatient unit [13].
In India, where the cancer issue is substantial, the QoL of cancer patients has not been sufficiently investigated, and most studies that are accessible have assessed QoL in connection to specific cancer types. In all these studies, cancer patients were consistently reported to have low QoL scores [16-19]. In two survey-based studies, the QoL scores were low and palliative care needs were significant among advanced cancer patients. This necessitates the adoption of interventions for optimal care and effective clinical management in cancer patients [20,21].
To fill this gap, a prospective interventional study is being conducted at the Centre of Excellence (CoE) established by AIIMS, Jodhpur, in collaboration with the India–Sweden Healthcare Innovation Centre. The study seeks to explore QoL as an important endpoint in evaluating the mental and social well-being of cancer patients receiving holistic cancer care at the CoE.
o Methodology
Study design and setting
This will be a single-arm, prospective, interventional study. The interventional component will include all standardof–care interventions required by cancer patients (surgery, radiation therapy, and medical oncology). The prospective component will include nutritional counseling, physical and rehabilitation therapy, psychological counseling, palliative care, and social welfare services under the Comprehensive Cancer Patient Support Services (CPSS) program. This study will be conducted for 12 months at the CoE established with collaboration between AIIMS, Jodhpur, and India–Sweden Healthcare Innovation Centre. The study has been approved by the Institutional Ethics Committee.
Study objectives
The study primarily aims to evaluate the impact of supportive care on QoL and various domain-specific measurements in cancer patients undergoing holistic care at the CoE.The secondary objectives include the assessment of patient profiles, treatment compliance, follow-up rates, treatment costs, and distress scores of patients and caregivers. A detailed description of the study objectives is provided in Box 1.
Box 1. Comprehensive Cancer Patient Supportive Services (CPSS) program objectives
Primary objectives:
■ To assess the QoL of cancer patients using validated global and site-specific tools of EORTC at the time of enrollment in the CPSS program (baseline) and during follow-ups.
■ To assess patients’ problems and needs in the specific domains of psychology, nutrition, physical and rehabilitation therapy, and palliative care.
■ To evaluate the changes in global QoL (EORTC QLQ-C30), site-specific QoL (EORTC), and various domain-specific measurements in patients undergoing supportive care treatment inthe CPSS program.
○ Secondary objectives:
■ To assess patient profiles in terms of demography, staging of cancer, treatment, comorbidity status, treatment effectiveness, and survival outcomes.
■ To assess treatment compliance and follow-up rates.
■ To assess the distress of patients and caregivers.
■ To assess the financial burden of disease.
QoL: Quality of life; EORTC: European Organization for Research and Treatment of Cancer; QLQ-C30: Quality of Life Questionnaire Core 30 Items.
Study population
The study participants will be adult patients (≥18 years) registered at AIIMS, Jodhpur, with a confirmed diagnosis of cancer and expected survival of at least 3 months. Registered patients undergoing radiation or chemotherapy for benign diseases and those unable to attend counseling sessions due to any physical or psychological disability will be excluded. Only patients who meet the inclusion criteria will be considered for enrollment in the study. As per estimates, 100 patients per month will be enrolled in the study.
CPSS program workflow
After enrollment, all patients will go through the CPSS program workflow, which will include baseline assessments and counseling sessions (Figure 1).
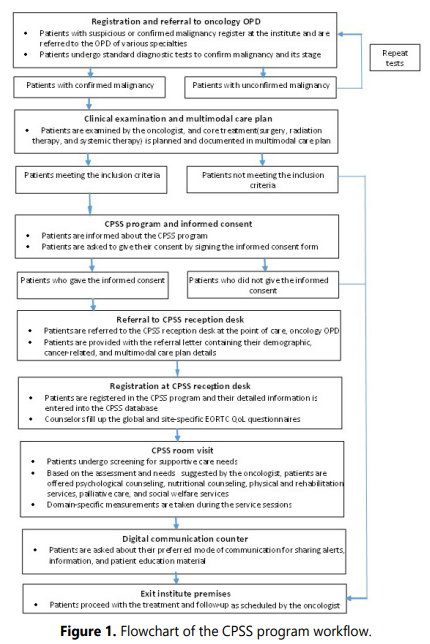
OPD: Outpatient department; CPSS: Cancer patient support services; EORTC: European Organization for Research and Treatment of Cancer; QoL: Quality of life.
Registration and referral to OPD
Patients with suspected malignancy or confirmed diagnosis of the same are eligible to register with the institute for physical or telemedicine consultation. Upon registration at the institute, the patients are referred to the oncology outpatient department (OPD) for various specialties. Patients reporting to the OPD undergo standard diagnostic check-ups for the confirmation and staging of their malignancy. Patients with confirmed malignancy will be given an appointment with the oncologist. Patients with unconfirmed malignancy will be advised to repeat the tests.
Clinical examination and referral to the CPSS program
Patients will be clinically examined by oncologists. Core treatments (surgery, radiation therapy, and systemic therapy) as per the standard of care will be scheduled and documented in the multimodal care plan. Following the care plan at the core oncology care, the patients fulfilling the inclusion criteria will be informed about the CPSS program and will be offered an informed consent form for enrolling in the program. Patients consenting to the same will be referred to the CPSS reception desk at the point of care, oncology OPD. The patients will be provided with referral letters containing basic identification details, type and stage of cancer, and a copy of the multimodal care plan from the core oncology care. Additionally, the referral letters will capture any specific indications, requests, or needs of the patients to be catered by the CPSS, as identified by the oncology team.
Registration in the CPSS program and room visit
All patients reporting at the CPSS reception desk will be registered in the CPSS program and details related to demographics, cancer, and multimodal care plan will be entered into a separate database. Counselors will be filling up the global European Organization for Research and Treatment of Cancer Quality of life Questionnaire (EORTC QLQ-C30) and site-specific QoL questionnaire for the registered patients. The registered patients will be examined by the counselors to ascertain their requirements for supportive care. Based on the counselor’s assessment and needs suggested by an oncologist, patients will be offered psychological counseling, nutritional counseling, physical and rehabilitation services, palliative care, and social welfare services. In addition to these services, patients will also be explained about their disease status, treatment, prognosis, and medication regimes. Patients will be motivated to treatment compliance and adherence to regular follow-ups. The domain-specific counselors will be handling the patients’ domain-specific measurements during the counseling sessions.
Digital communication counter
Patients will be asked about their preferred forms of communication—SMS, email, WhatsApp, or telephone calls— for sharing regular alerts, information, and patient education materials.
End of workflow
After the completion of the workflow, patients will exit the CoE premises and proceed with the treatment and follow-up as scheduled by the oncologist.
CPSS program follow-up
After the baseline assessment and counseling, patients will revisit the CPSS workflow regularly throughout their treatment or at one of the time points synchronized with follow-up with individual counselors, systemic therapy visits (weekly thrice for chemotherapy), or follow-up scheduled by oncologists.
Data collection and outcome measurement
Demographic, patient-specific, cancer-specific, and multimodal care plan-related data will be stored in computerized health records. Global (EORTC QLQ-C30) and site-specific (EORTC) QoL questionnaires will be used as measurement tools to assess the QoL of patients at the time of enrollment (baseline) and follow-up visits. EORTC assessments will be captured at least every 3 months. Domain--specific measurements will be recorded during counseling sessions to assess the domain-specific changes.
EORTC Quality of Life Questionnaire Core 30 Items
The EORTC QLQ-C30 is a questionnaire developed to assess the QoL of cancer patients [22,23]. It is accompanied by disease-specific modules that evaluate extra symptoms and QoL issues unique to various types of cancer. The EORTC QLQ-C30 includes functional scales (physical, role, cognitive, emotional, and social), symptom scales (fatigue, pain, nausea, and vomiting), global health status and QoL scale, as well as several single-item symptom assessments. The item is scaled from 1 (not at all) to 4 (very much), or from 1 (extremely poor) to 7 (excellent). The scores range from 0 to 100. Higher scores on functional and global QoL scales indicate higher degrees of functioning. A higher score on symptom-oriented scales indicates more serious symptoms. EORTC QLQ-C30 has been shown to have acceptable validity and reliability and the ability to distinguish patients according to their performance status [16-18, 24].
Statistical analysis
The analysis will include all variables captured in the patients’ data according to the protocol. Descriptive statistics will be performed to describe the demographics of the study population. It will be presented in the form of continuous and categorical variables. For normally distributed continuous variables, means and standard deviation will be calculated, and for non-normally distributed continuous variables, medians and interquartile ranges will be calculated. Continuous variables will be compared using a t-test and analysis of variance. Categorical variables will be expressed as percentages and compared using chi-square and Fischer exact test. The association between the mean score of QoL and the demographic variables, such as types and stages of cancer, will be determined using one-way ANOVA. Statistical significance will be considered at p<0.05. Data analysis will be done using standard statistical software.
Expected outcomes
The most likely outcome will be an improvement in QoL scores (global as well as site-specific) and domain-specific parameters in cancer patients from the time of enrollment to the follow-up visits. The findings from this study will help to provide information about the possible effect of cancer and its treatment on the functioning and well-being of patients, identify common problems faced by patients, and develop appropriate interventions to overcome these problems in the Indian settings. These findings may be useful for future research and management of patients diagnosed with cancer in developing countries such as India.
Conclusion
This study attempts to evaluate the outcomes of a holistic care approach that aims to provide supportive care (psychological counseling, nutrition counseling, physical and rehabilitation services, palliative care, and social welfare services) alongside conventional treatments (surgery, radiation therapy, and chemotherapy) for adult cancer patients under one roof. The primary goal of the study is to evaluate the impact of outcomes on the QoL of patients and to assess how these outcomes may influence the management of cancer patients. The findings of the study will facilitate the routine use of QoL assessment as a part of clinical practice in cancer patients receiving treatment at various institutes across the country.
Acknowledgement: The authors would like to thank BioQuest Solutions for medical writing support, which was funded by India-Sweden Healthcare Innovation Centre. The manuscript was developed in accordance with GPP 2022 guidelines (https://www.ismpp.org/gpp-2022).
Financial Support: Supported by India-Sweden Healthcare Innovation Centre
Conflicts of interest disclosure: None declared
Authors’ Contribution: All authors have contributed equally to the design, conception, drafting, review and finalization of manuscript.
References
- WHO. Cancer. 2022; Accessed Feb 21, 2022
- Ferlay J, Colombet M, Soerjomataram I, et al. Cancer statistics for the year 2020: An overview. Int J Cancer. 2021. doi: 10.1002/ijc.33588
- Globocan India; Global Cancer Observatory. 2020.
- NCDIR. Report of National Cancer Registry Programme (ICMRNCDIR), Bengaluru, India. 2020.
- Ramasubbu SK, Pasricha RK, Nath UK, Rawat VS, Das B. Quality of life and factors affecting it in adult cancer patients undergoing cancer chemotherapy in a tertiary care hospital. Cancer Rep. 2021; 4(2): e1312. doi: 10.1002/cnr2.1312
- Evans Webb M, Murray E, Younger ZW, Goodfellow H, Ross J. The supportive care needs of cancer patients: A systematic review. J Cancer Educ. 2021; 36(5): 899-908. doi: 10.1007/s13187-020-01941-9
- Wang T, Molassiotis A, Chung BPM, Tan JY. Unmet care needs of advanced cancer patients and their informal caregivers: a systematic review. BMC Palliat Care. 2018; 17(1): 96. doi: 10.1186/s12904-018-0346-9
- Popescu RA, Roila F, Arends J, Metro G, Lustberg M. Supportive care: Low cost, high value. Am Soc Clin Oncol Educ Book. 2021; 41: 1-11. doi: 10.1200/EDBK_320041
- Ravasco P. Nutrition in cancer patients. J Clin Med. 2019; 8(8): 1211. doi: 10.3390/jcm8081211
- Medeiros KS, Queiroz JF, Monteiro MN, et al. Impact of mobile applications on adherence to cancer treatment: a systematic review and meta-analysis protocol. BMJ Open. 2019; 9(11): e027246. doi: 10.1136/bmjopen-2018-027246
- Alam MM, Rahman T, Afroz Z, et al. Quality of Life (QoL) of cancer patients and its association with nutritional and performance status: A pilot study. Heliyon. 2020; 6(10): e05250. doi: 10.1016/j.heliyon.2020.e05250
- Jacobsen PB, Jim HS. Consideration of quality of life in cancer survivorship research. Cancer Epidemiol Biomarkers Prev. 2011; 20(10): 2035-2041. doi: 10.1158/1055-9965.EPI-11-0563
- Scotte F. The importance of supportive care in optimizing treatment outcomes of patients with advanced prostate cancer. Oncologist. 2012; 17(Suppl 1): 23-30. doi: 10.1634/theoncologist.2012-S1-23
- Faller H, Hass HG, Engehausen D, Reuss-Borst M, Wockel A. Supportive care needs and quality of life in patients with breast and gynecological cancer attending inpatient rehabilitation. A prospective study. Acta Oncol. 2019; 58(4): 417-424. doi: 10.1080/0284186X.2018.1543947
- MASCC. Multinational Association of Supportive Care in Cancer. Accessed Feb 23, 2022
- Parkar S, Sharma A, Shah M. Exploring quality of life among headand-neck cancer patients in Western India using European organization for research and treatment of cancer questionnaires. J Cancer Res Therapeutics. 2022, 18(4): 990-9966. doi: 10.4103/jcrt.JCRT_450_20
- Parmar V, Badwe RA, Hawaldar R, et al. Validation of EORTC quality-oflife questionnaire in Indian women with operable breast cancer. Natl Med J India. 2005; 18(4): 172-177.
- Rao VV, Shaikh SM, Bhat M, Aramani A, Lobo V. Quality of Life of Head-and-Neck Cancer Patients – Reliability and Effectiveness of the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire-30 and European Organization for Research and Treatment of Cancer. Quality of Life Questionnaire-H and N35 Questionnaires in Patients in a Tertiary Care Center in India. Ann Indian Acad Otorhinolaryngol Head Neck Surg. 2017; 1(2): 22-25. doi: 10.4103/aiao.aiao_2_18
- Jyani G, Chauhan AS, Rai B, Ghoshal S, Srinivasan R, Prinja S. Healthrelated quality of life among cervical cancer patients in India. Int J Gynecol Cancer. 2020; 30(12): 1887-1892. doi: 10.1136/ijgc-2020-001455
- Asthana S, Bhatia S, Dhoundiyal R, Labani SP, Garg R, Bhatnagar S. Quality of life and needs of the Indian advanced cancer patients receiving palliative care. Cancer Res Stat Treat. 2019; 2: 138-144. doi: 10.4103/0973-1075.63133
- Nayak MG, George A, Vidyasagar MS, et al. Quality of life among cancer patients. Indian J Palliat Care. 2017; 23(4): 445-450. doi: 10.4103/IJPC.IJPC_82_17
- EORTC quality of life. EORTC quality of life questionnaires 2011. Accessed Feb 22, 2022
- Chaukar DA, Das AK, Deshpande MS, et al. Quality of life of head and neck cancer patient: validation of the European organization for research and treatment of cancer QLQ-C30 and European organization for research and treatment of cancer QLQ-H&N 35 in Indian patients. Indian J Cancer. 2005; 42(4): 178-184
